What Matters Most
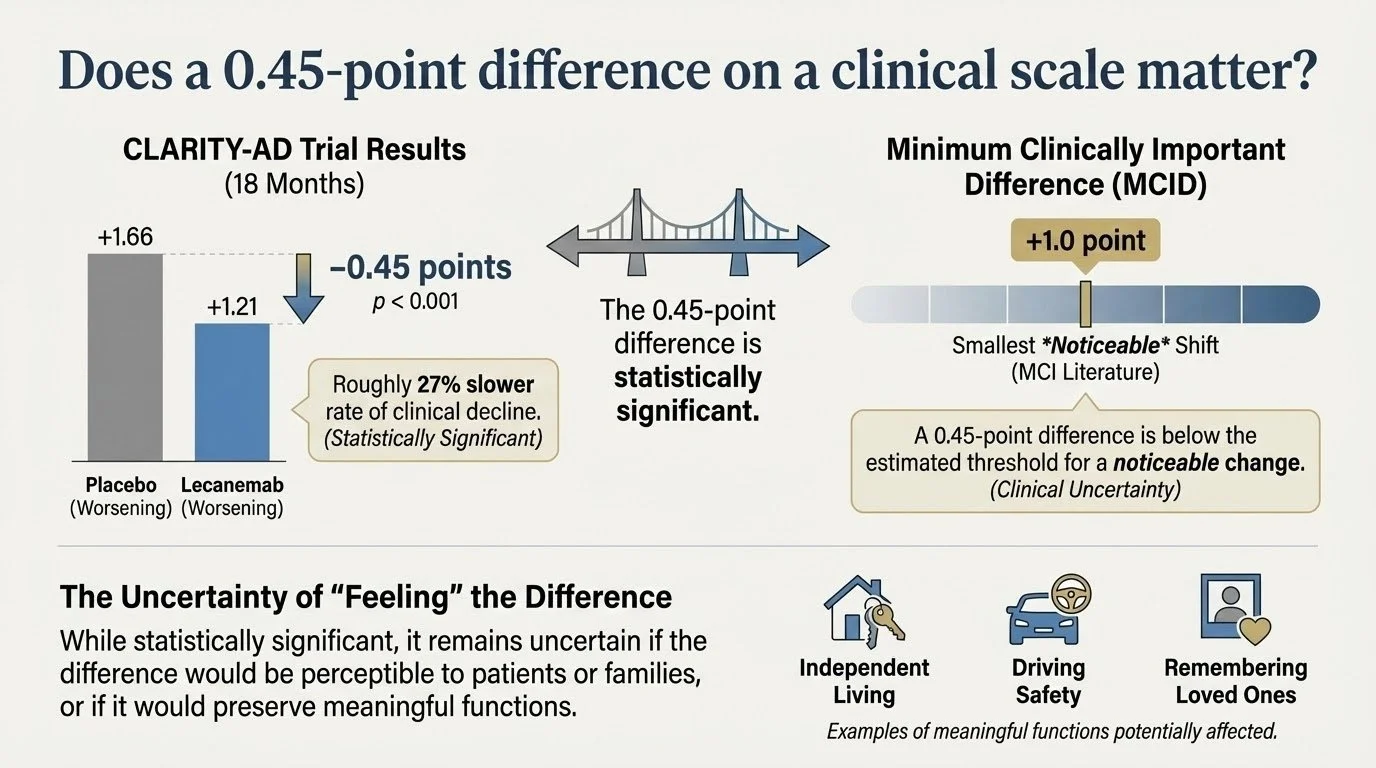
Does a 0.45-point difference on a clinical scale matter?
In the Phase 3 CLARITY-AD trial of lecanemab, patients with early Alzheimer’s disease treated with the drug had a mean change in CDR-SB of ≈ +1.21 at 18 months versus +1.66 on placebo (difference ≈ –0.45 points, p <0.001) — representing roughly a 27% slower rate of clinical decline.
Is a –0.45-point difference meaningful to a person or family? The minimum clinically important difference (MCID) literature suggests that, in MCI populations, a change of about +1 point on CDR-SB may represent the smallest shift likely to be noticeable.
In other words: while the result is statistically significant, it remains uncertain whether every individual would “feel” the difference, whether their family would observe it, or whether meaningful functions (e.g., independent living, driving safety, remembering loved ones) would be preserved.
Would this difference be noticeable in your daily life?
Would you feel different?
Would your family see a difference?
Would it preserve what you're terrified of losing?
The honest answer: We don't know.
What Clinical Trials Typically Measure:
CDR-Sum of Boxes scores (clinician ratings of thinking and function)
Amyloid plaque levels in the brain (measured by blood biomarkers and PET scans)
Cognitive test performance
Global clinical impression (clinician's rating of overall severity)
What Patients and Families Say Matters Most (in order):
Improving or restoring memory
Stopping disease progression
Slowing disease progression
Improving ability to do everyday tasks
Remembering family members
Remaining independent and not feeling like a burden
Removing plaques and tangles from the brain
Notice what's at the bottom? Removing amyloid plaques.
Notice what's missing entirely? The scales clinical trials use don't directly measure most of what patients care about: remembering loved ones' faces, not feeling like a burden, maintaining independence.
The 0.45-Point Question
Let's return to lecanemab's 0.45-point difference on the CDR-SB scale over 18 months.
Is 0.45 points meaningful?
The research community: Maybe. One expert panel suggested 0.5-1.0 points in a single domain (like memory) could be meaningful if caught early enough.
Patients and families: We don't know.
Does it mean:
Mom will remember my name for an extra 6 months?
Dad can balance his checkbook a bit longer?
My spouse won't need 24/7 care quite as soon?
I'll have more "good days" when I feel like myself?
These are the questions that matter and clinical trials typically don’t.
What "Clinically Meaningful" Should Mean
A 2025 workshop report proposed a new framework for defining meaningful outcomes in Alzheimer's trials:
1. Patient-Centered Outcomes Must Be Primary
Not secondary endpoints or exploratory analyses—primary. Trials should measure:
Patient-reported quality of life
Ability to perform activities that matter to the individual (hobbies, social engagement, self-care)
Caregiver burden and quality of life (disease affects the whole family)
Time to critical milestones (loss of independence, residential transition, loss of specific abilities)
2. "Minimal Clinically Important Difference" Must Reflect Patient Perspective
Currently, experts define thresholds like "1-2 CDR-SB points is meaningful." But meaningful to whom?
Better approach: Ask patients and families experiencing different levels of decline: "How much improvement or slowing would need to occur for you to consider treatment worthwhile given the risks, costs, and burdens?"
This is called anchoring to patient global impression of change—linking statistical measures to what people actually feel and notice.
3. Time Savings Must Be Interpretable
How many months of progression are delayed?
For example:
"Lecanemab provides approximately 5-7 months of delay in progression over 18 months of treatment"
"This means remaining at your current level of function about 5-7 months longer than you would without treatment"
This is interpretable. Patients can weigh: "Is 5-7 months of preserved function worth 18 months of infusions, MRI monitoring, risk of brain swelling, and cost?"
Different people will answer differently—and that's okay. The point is informed decision-making based on outcomes that matter.
Long-Term Economic Value
Modeling shows that even modest slowing of decline creates long-term value:
Scenario 1: 18 months of lecanemab, 27% slowing
Increased lifetime quality-adjusted life years (QALYs)
Reduced informal caregiving hours
Medical cost savings from delaying severe dementia stage
Net value: ~$40,000-60,000 per patient over lifetime
Scenario 2: 48 months of treatment, 50% slowing (hypothetical future treatment)
Dramatically increased QALYs
Years of delayed nursing home placement
Preserved workforce participation for both patient and caregiver
Net value: ~$150,000-200,000 per patient over lifetime
The insight: Even small effects compound over time. A 25% slowing may not seem dramatic year-to-year, but over 5-10 years could mean:
1-2 extra years living at home vs. nursing facility
1-2 extra years employed (for early-onset patients)
1-2 extra years when family caregivers don't need to quit jobs
Delayed transition to 24/7 care needs
But these benefits aren't captured in 18-month trials measuring CDR-SB scores.
People Are Complex
Research establishing Alzheimer's biomarkers has largely been conducted in select populations.
The problem:
Biomarkers (amyloid, tau) may be less strongly associated with cognitive decline in some people
Why? Likely because other factors contribute more to cognitive impairment:
Vascular disease from uncontrolled hypertension and diabetes
Social determinants of health (education quality, socioeconomic status)
Mixed pathologies (not pure Alzheimer's but combined pathologies)
Translation: What's "clinically meaningful" may differ depending on the person.
What This Means for Cognitive Stewardship
1. We Must Ask What Matters to YOU
In initial consultations, I ask:
What abilities are you most afraid of losing?
What would "success" look like for a treatment?
What trade-offs are you willing to accept (burden, cost, risk) for how much benefit?
What defines quality of life for you right now?
These answers guide everything: Whether to pursue treatments, which risk factors and lifestyle interventions to prioritize and how aggressive you should be, when to initiate legal planning.
2. We Must Measure What Matters
In addition to cognition, Cognitive Stewardship measures:
Functional capacity across domains (financial, medication management, driving, meal preparation)—the IADLs that patients prioritize
Patient-reported quality of life and sense of well-being
Care partner burden and family impact
Preservation of meaningful activities (hobbies, social connections, independence)
Time to critical milestones (independent living, drive safely, manage finances)
Every 6 months, we assess: Are you maintaining the abilities that matter most to you? Is quality of life preserved? Is family coping?
This tells us whether interventions are working in ways that matter—not just whether CDR-SB changed by 0.5 points.
3. We Must Translate Science into Lived Experience
I don't tell patients: "Your CDR-SB score increased 1.5 points over the past year."
I say: "Your memory and problem-solving have declined to a level where managing finances independently is becoming risky. Last year, you could balance your checkbook and detect errors. Now, you're missing bills and making calculation mistakes. This suggests we should implement financial protections like joint account management and power of attorney activation."
I don't say: "Lecanemab slows decline by 0.45 CDR-SB points over 18 months."
I say: "Lecanemab might give you about 5-7 months longer at your current level of function—meaning abilities like driving, managing your home, and participating in hobbies might be preserved a bit longer. We'd need to weigh this modest benefit against biweekly infusions, brain swelling risk, and costs. What feels right to you?"
This is patient-centered communication—translating research findings into terms that enable informed decisions.
4. We Must Empower Patients with Their Own Data
The Study Participant Bill of Rights says patients deserve their research results. Cognitive Stewardship goes further: You deserve results explained in context, with action plans, and with continuity of expertise.
You're not a data point. You're a partner in managing your cognitive health.
The Bottom Line: Ask the Right Questions
The next time you read a headline about an Alzheimer's drug showing "statistically significant benefit," ask:
Benefit for what outcome?
Meaningful to whom?
How would this feel in daily life?
Is this what patients and families are hoping for?
The 0.45-point CDR-SB difference isn't inherently meaningful or meaningless. Context makes it meaningful:
To a 68-year-old woman terrified of forgetting her grandchildren, 5-7 months of preserved memory might be priceless—worth the infusions and risks.
To an 82-year-old man who values quality over quantity and hates medical procedures, modest slowing may not justify treatment burden.
Both are valid. The problem is we don't have the data to help people make truly informed choices aligned with their values.
Cognitive Stewardship fills the gap—measuring what matters, translating science into lived experience, and empowering you to make decisions aligned with your priorities.
References
van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in Early Alzheimer's Disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
Andrews JS, Desai U, Kirson NY, et al. Disease Severity and Minimal Clinically Important Differences in Clinical Outcome Assessments for Alzheimer's Disease Clinical Trials. Alzheimers Dement (N Y). 2019;5:354-363. doi:10.1016/j.trci.2019.06.005
Stoeckel LE, Fazio EM, Hardy KK, Kidwiler N, McLinden KA, Williams B. Clinically Meaningful Outcomes in Alzheimer's Disease and Alzheimer's Disease-Related Dementias Trials. Alzheimers Dement (N Y). 2025;11(1):e70058. doi:10.1002/trc2.70058
What Would You Change?
The Diagnostic Breakthrough
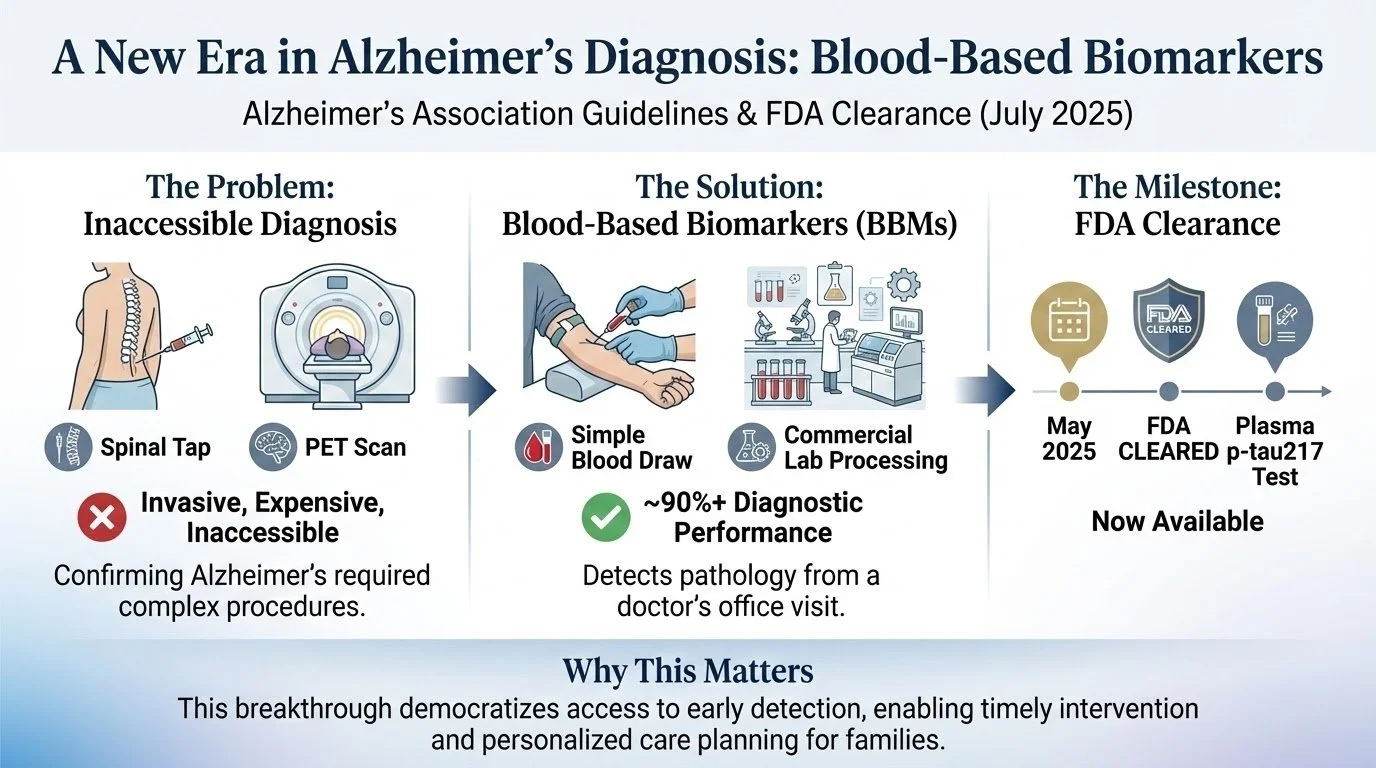
On July 28, 2025, the Alzheimer's Association released clinical practice guidelines recommending how specialty clinicians should use blood-based biomarkers (BBMs).
Why this matters: Until now, confirming Alzheimer's disease required either a lumbar puncture (spinal tap) to analyze cerebrospinal fluid or a PET scan. Both are invasive, expensive, and inaccessible to many families. Now, a simple blood test—drawn at your doctor's office, processed by commercial labs—can detect Alzheimer’s pathology with ~90%+ diagnostic performance in peer-reviewed studies (exact performance varies by assay and population). In May 2025, FDA cleared the first blood test measuring plasma p-tau217 and it is now available.
Do you want to know?
The Question No One Is Asking
Doctors are asking:
"Should we order the test?"
Researchers are asking:
"How accurate is it?"
Insurance companies are asking:
"Will we cover it?"
But the most important question for families is:
What would you change if you knew you had Alzheimer's pathology in your brain?
Not "what can be done"—what would YOU do differently?
What It Means to Know
You have Alzheimer's pathology—amyloid plaques and tau tangles—accumulating in your brain right now.
It does NOT mean:
You will definitely develop dementia (some people with pathology never progress)
You will decline rapidly (timeline is unpredictable—could be 2 years, could be 20)
Your fate is sealed (interventions can slow progression)
You should panic
What it DOES mean is that a door has opened to early intervention when new treatments are available and when lifestyle intervention works best. A door to legal planning while you have full capacity. A door to decisions that become more difficult later. A door to preparing your family before crisis.
The New Disease-Modifying Therapies
Lecanemab and donanemab—FDA-approved drugs that slow Alzheimer's progression by about 25%—have strict eligibility requirements:
✅ Mild cognitive impairment OR mild dementia
✅ Confirmed amyloid pathology (requires biomarker test)
❌ NOT moderate or severe dementia
Translation: If you wait until symptoms are obvious, you're likely ineligible. The treatment window closes at moderate dementia.
The Lifestyle Intervention Evidence
The FINGER trial in Finland and US POINTER trial (2025) proved that intensive multi-domain lifestyle interventions can slow cognitive decline. The Lancet Commission (2024) reported 14 modifiable risk factors for dementia. Higher physical activity is associated with slower cognitive and functional decline in individuals with elevated baseline amyloid. Critical finding: Benefits are greatest when started in the MCI stage or earlier. Once moderate dementia arrives, lifestyle interventions are much less effective for patients, but become more important for managing caregiver stress and well-being.
Approaches Providers Can Take Right Now
Approach 1: "Test Everyone with Symptoms"
The problem: Testing without infrastructure to support results. Knowledge without guidance. Diagnosis without stewardship.
Approach 2: "Don't Test Unless It Changes Management"
The problem: Avoidance doesn't prevent progression—it just prevents preparation. The "wait and see" approach guarantees missing treatment windows.
There's a Third Approach: Decision-Preparedness Testing
The question isn't "should we test?" The question is: "What would we do with results?"
"If the test shows Alzheimer's pathology, what would you do?"
Would you pursue disease-modifying therapy?
Would you intensify lifestyle interventions?
Would you accelerate legal and financial planning?
Would you have family conversations about the future?
Would you consider clinical trial participation?
"What are your biggest fears about knowing?"
Anxiety about the future?
Impact on relationships or self-identity?
Discrimination concerns (employment, insurance)?
Not knowing how to act on results?
If your list has 3+ items, have a conversation about testing. Tests are best acted on in specialty care or within a defined care pathway, per the AA guideline.
What To Do Next
If you or a family member has cognitive concerns:
1. Seek Expert Evaluation (Not Just Primary Care Screening)
Primary care doctors are excellent at many things, but detailed cognitive assessment and BBMs interpretation require specialized expertise
See a neuropsychologist, neurologist, or geriatrician with cognitive disorders expertise
Insist on comprehensive evaluation, not just MoCA or MMSE (too insensitive for early changes)
2. Don't Go It Alone
Cognitive decline is a family journey—involve spouse, adult children, trusted friends
Seek services that provide longitudinal support, not just episodic evaluation
Consider programs like Cognitive Stewardship that offer continuous monitoring and decision coaching
3. Act on Results
If biomarker-positive: Immediately begin evidence-based interventions (lifestyle optimization, DMT evaluation if appropriate, advance planning)
If biomarker-negative: Pursue alternative diagnoses and address modifiable factors
Don't let positive results cause paralysis—this is where expert guidance is critical
4. Stay Informed
Biomarker science is evolving rapidly—guidelines will update
Clinical trials are ongoing—opportunities for cutting-edge treatment
New therapies in pipeline—tau-targeting drugs, anti-inflammatory agents, combination therapies
The window for intervention is open. The tools for early detection are here. The question is: Will you use them?
Early Detection Is Only Valuable If Followed by Action
The 2025 Alzheimer's Association guidelines on BBMs represent a pivotal moment in the fight against Alzheimer's disease. For the first time, we can detect pathology early, accurately, and accessibly.
Some experts believe direct-to-consumer or at-home Alzheimer’s blood biomarker testing may be “an innovation too far” — meaning it may cause more harm (anxiety, misinterpretation, unnecessary follow-up tests, discrimination) than benefit in the current state.
They want:
Better care infrastructure: Legal protections against discrimination for biomarker-positive individuals; more clinicians trained in dementia/Alzheimer’s care.
Funding & workforce expansion: More specialists need to be trained and available.
Verified treatments in asymptomatic people: Tests only make sense when there are actionable interventions for people who test positive but do not have symptoms.
This is why I created Cognitive Stewardship. The science of early detection has advanced faster than the clinical infrastructure to support it. Families are getting biomarker results without guidance to know what’s next.
We close that gap.
If you or a loved one has cognitive concerns, or if you've received biomarker results and aren't sure what to do next, Treasure Coast Cognition is here to help.
References
Alzheimer's Association. Appropriate Use of Blood-Based Biomarkers in Alzheimer's Disease: Clinical Practice Guideline From the Alzheimer's Association. Alzheimers Dement. 2025. Published online July 28, 2025. doi:10.1002/alz.14225
Labcorp. Labcorp Launches First FDA-Cleared Blood Test for Alzheimer's Disease. Published May 2025.
Yaffe K, Barnes DE, Rosenberg D, et al. Effect of a Multidomain Lifestyle Intervention vs Health Education on Cognitive Function in Older Adults at Increased Risk of Alzheimer Disease: The US POINTER Randomized Clinical Trial. JAMA. 2025;333(3):217-229. doi:10.1001/jama.2024.24157
Livingston G, Huntley J, Liu KY, et al. Dementia Prevention, Intervention, and Care: 2024 Report of the Lancet Standing Commission. Lancet. 2024;404(10452):572-628. doi:10.1016/S0140-6736(24)01296-0
Rabin JS, et al. Physical Activity and Longitudinal Cognitive and Functional Decline in Alzheimer Disease. Nat Med. 2025. doi:10.1038/s41591-025-03955-6
Personalized Prevention: Targeting Modifiable Risk Factors in Cognitive Stewardship
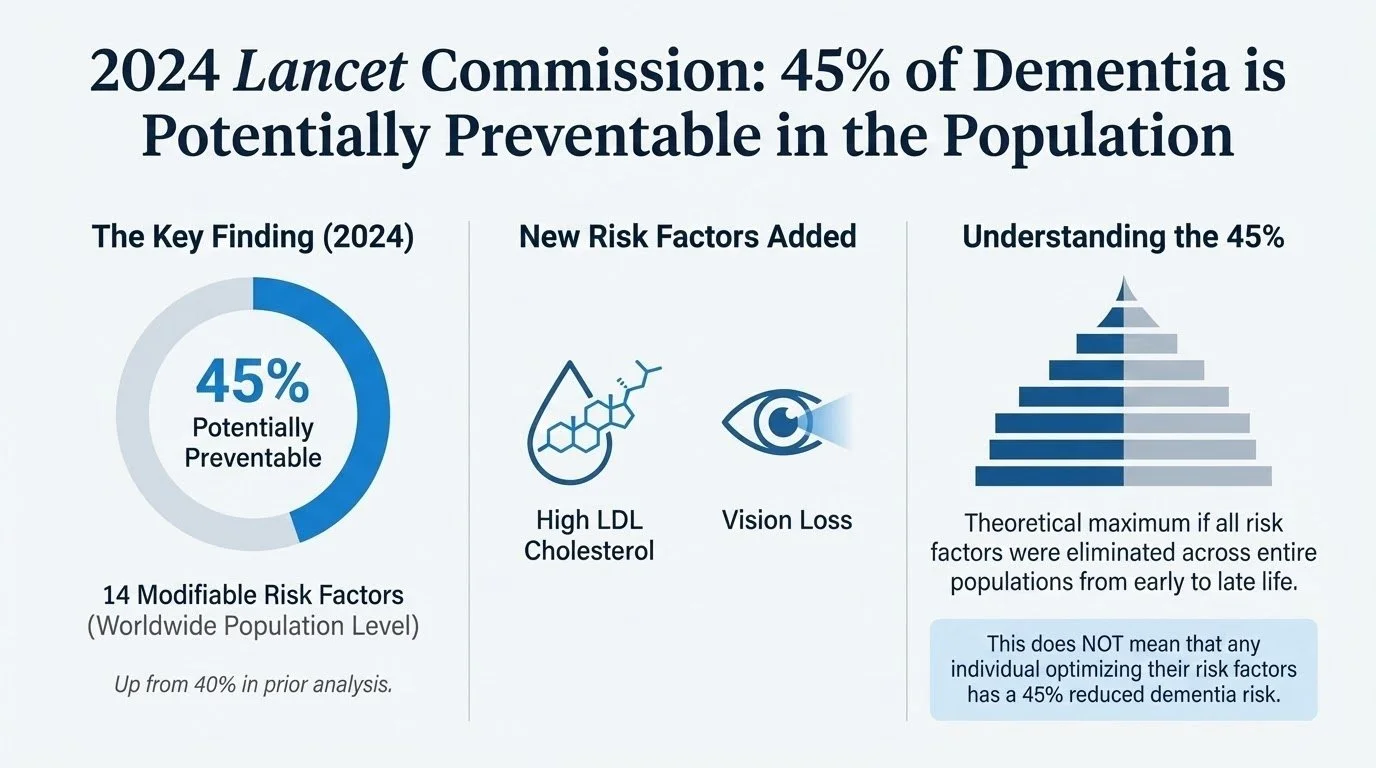
2024 Lancet Commission: 45% of Dementia is Potentially Preventable in the Population
The 2024 Lancet Commission on dementia prevention now identifies 14 modifiable risk factors that collectively account for 45% of dementia cases worldwide—up from 40% in the prior analysis with the addition of high LDL cholesterol and vision loss.
45% represents the theoretical maximum if all risk factors were eliminated across entire populations from early life through late life. This does NOT mean that any individual optimizing their risk factors has a 45% reduced dementia risk.
Midlife Interventions May Be Most Critical
The majority of modifiable risk burden (approximately 60% of the 45%) occurs in midlife when vascular and metabolic risk factors exert their greatest impact on brain health decades later.
Life-Course Risk Factor Model
Early Life (ages <45):
Less education (5%) - Limited cognitive stimulation and cognitive reserve building in formative years
Midlife (ages 45-65):
Hearing loss (7%) - The single largest modifiable risk factor
High LDL cholesterol (7%) - NEW for 2024; midlife dyslipidemia accelerates vascular brain changes
Depression (3%) - May be both risk factor and early symptom
Traumatic brain injury (3%) - Even mild TBI increases long-term dementia risk
Physical inactivity (2%) - Sedentary lifestyle deprives brain of neurotrophic benefits
Diabetes (2%) - Chronic hyperglycemia damages cerebral microvasculature
Smoking (2%) - Vascular damage and oxidative stress
Hypertension (2%) - Uncontrolled BP in midlife drives white matter disease
Obesity (1%) - Metabolic syndrome and chronic inflammation
Excessive alcohol (1%) - >21 units/week associated with brain atrophy
Late Life (ages >65):
Social isolation (5%) - Lack of cognitive stimulation and increased depression risk
Air pollution (3%) - Fine particulate matter (PM2.5) exposure causes neuroinflammation
Vision loss (2%) - NEW for 2024; untreated cataracts and poor vision reduce engagement
2025 US POINTER Trial: Lifestyle Prevention
Published January 2025 in JAMA, the US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk (POINTER) trial represents the first large-scale validation of the Finnish FINGER model in Americans.
Key Findings
Primary Outcome - Global Cognitive Composite: equivalent to 1-2 years of preserved cognitive function
Critical Insights: Any lifestyle intervention, even minimal, provides benefit. However, structured programs deliver ~30% greater cognitive gains (0.24 vs. 0.21 SD/year improvement). The program works, but only if people actually do it. Cognitive Stewardship provides care coordination and evidence-based strategies adherence strategies for maintenance of behavior change to slow decline, not prevent dementia.
Cognitive Stewardship can help translate the Lancet Commission's 14 modifiable risk factors and the US POINTER trial's structured intervention model into a personalized, sustainable program for your brain health. Through continuous monitoring, expert guidance, and intensive support, we can help you implement these evidence-based strategies proven to slow cognitive decline—while also navigating the 10 critical decision points where expert guidance prevents costly mistakes. You get both: (1) Personalized lifestyle intervention for cognitive protection, and (2) Decision-preparedness coaching for life transitions. Together, these maximize your cognitive trajectory and quality of life.
References
Livingston G, Huntley J, Liu KY, et al. Dementia Prevention, Intervention, and Care: 2024 Report of the Lancet Standing Commission. Lancet. 2024;404(10452):572-628. doi:10.1016/S0140-6736(24)01296-0
Yaffe K, Barnes DE, Rosenberg D, et al. Effect of a Multidomain Lifestyle Intervention vs Health Education on Cognitive Function in Older Adults at Increased Risk of Alzheimer Disease: The US POINTER Randomized Clinical Trial. JAMA. 2025;333(3):217-229. doi:10.1001/jama.2024.24157
The Healthcare System Isn’t Ready
A colleague was at her primary care visit. She asked how to get blood-based biomarker testing at a major university medical center (where she sees her doctors), and was told that she could try to go through neurology but at her age it was basically impossible. Maybe the response would have been different if she were older, but it struck her that even those proactive about getting tested face significant barriers.
Even at top medical centers, proactive families face impossible barriers:
You can't get blood biomarker testing because you're "too young" or "not symptomatic"—despite tests that predict dementia 10 years before symptoms appear.
Your primary care doctor waits for obvious memory problems before acting—by then, treatment eligibility windows have already narrowed dramatically.
Specialist referrals take 3-6 months. Eligibility testing takes another 2 months. By the time traditional care pathways respond, half of early dementia patients have already progressed beyond treatment eligibility.
Healthcare system delays happen when you need action.
Cognitive Stewardship changes this.
We help families act years earlier—with proactive monitoring, personalized intervention, and access when concerns emerge—so you can intervene when science shows it matters most.
The Waiting Years
The Waiting Years.
A friend reached out.
She told me about her mother.
October 2023: The family noticed changes. Memory issues. Movement struggles. They called the university memory clinic — the one everyone recommends.
First available appointment: September 2024.
So they found a physician’s assistant in another city. Tried there. The physician’s assistant was doing their best. The answers didn’t fit what the family was seeing.
By the time they finally reached the specialist and got a DaTscan ordered, it was August 2025.
How hard is it to get imaging?
MRI: Easy.
DaTscan: Not easy.
Real-world barriers:
• Insurance approval: weeks to months
• Limited centers
• 6–12 month wait times
• Some neurologists wait until symptoms are “obvious enough”
Meanwhile, families wait.
Nearly two years from first noticing changes to getting the right diagnosis.
Not because they didn’t care.
Not because they didn’t try.
Because the system isn’t built for the early stage.
In those two years, they navigated alone:
Is this normal aging?
Should we push for different tests?
Which supplements matter?
When do we get a walker? A shower chair?
How do we find the right support?
Where do we find support?
My friend is a researcher. She did everything right. She dug through forums, found Zoom groups, paid thousands for a “personalized” program that delivered generic guidance.
She told me:
“I would have paid anything to not wait. Not for a cure — just for someone who knew what to ask for and when.”
That gap — between noticing something is wrong and getting meaningful support — is where families lose time.
Cognitive Stewardship™ can help.
Not to replace your medical team.
Not to diagnose alone.
To guide families through the waiting — the uncertainty, the decisions, the system navigation.
To make sure that when they finally reach the specialist, they haven’t lost two years.
If you’ve lived this — the waiting, the confusion, the “I wish someone had told us” — what did you need most?
I’m building this for the families who shouldn’t have to navigate alone.
Please share your story. Your experiences are shaping this work.
The views expressed here are my own and do not represent those of the NIH or the U.S. government.